
A landmark 2025 systematic review and meta-analysis published in JAMA Network Open — encompassing 376 studies and 347,468 individuals with chronic pain from 50 countries — found that approximately 40% of adults with chronic pain mental health treatment have clinically significant depression and approximately 40% have clinically significant anxiety. A separate 2024 study published in the journal PAIN by De La Rosa et al. at the University of Arizona found that unremitted anxiety and depression symptoms are five times more common among people with chronic pain than among those without. These are not two separate problems that happen to coexist.
They are deeply interconnected — sharing neurobiological pathways, amplifying each other, and requiring integrated treatment. At Arizona Pain and Spine Institute in Mesa, Dr. Asim Khan and Dr. Daniel Ryklin treat both chronic pain conditions and mental health conditions like PTSD and anxiety under one roof — an approach the research increasingly shows is essential for the best outcomes.
The Numbers: How Common Is the Pain-Mental Health Connection?
The scale of this problem is staggering, and the data has become sharper in recent years.
According to the CDC’s National Center for Health Statistics (NCHS Data Brief No. 518, November 2024), 24.3% of U.S. adults — roughly 1 in 4 — had chronic pain in 2023. Among those, 8.5% had high-impact chronic pain that frequently limited life or work activities. The CDC’s 2023 MMWR (Rikard et al.) explicitly links chronic pain mental health treatment to “increased anxiety and depression” and “unmet mental health needs.”
The JAMA Network Open meta-analysis (Aaron et al., 2025) provides the most comprehensive data to date on the mental health burden within chronic pain populations. After analyzing 376 studies spanning a decade of research across 50 countries, the researchers found pooled prevalence rates of 39.3% for depression and 40.2% for anxiety among adults with chronic pain. The prevalences were highest among people with fibromyalgia and among samples that were younger and predominantly female.
Get Back Your Normal Life Again
As pain specialists, we can guarantee that we are more than qualified in alleviating your pain and treating your condition.
The University of Arizona PAIN journal study (De La Rosa et al., 2024) used nationally representative data from the National Health Interview Survey and found that nearly 1 in 20 U.S. adults experience the co-occurrence of chronic pain and anxiety or depression. The study found that this co-occurrence results in substantial functional limitations in daily activities and that people living with both conditions had significantly worse outcomes than those with either condition alone.
Why Pain and Mental Health Are Biologically Connected
Understanding why chronic pain and mental health conditions so frequently co-occur requires looking at the underlying biology — and it explains why treating only one side of the equation often fails.
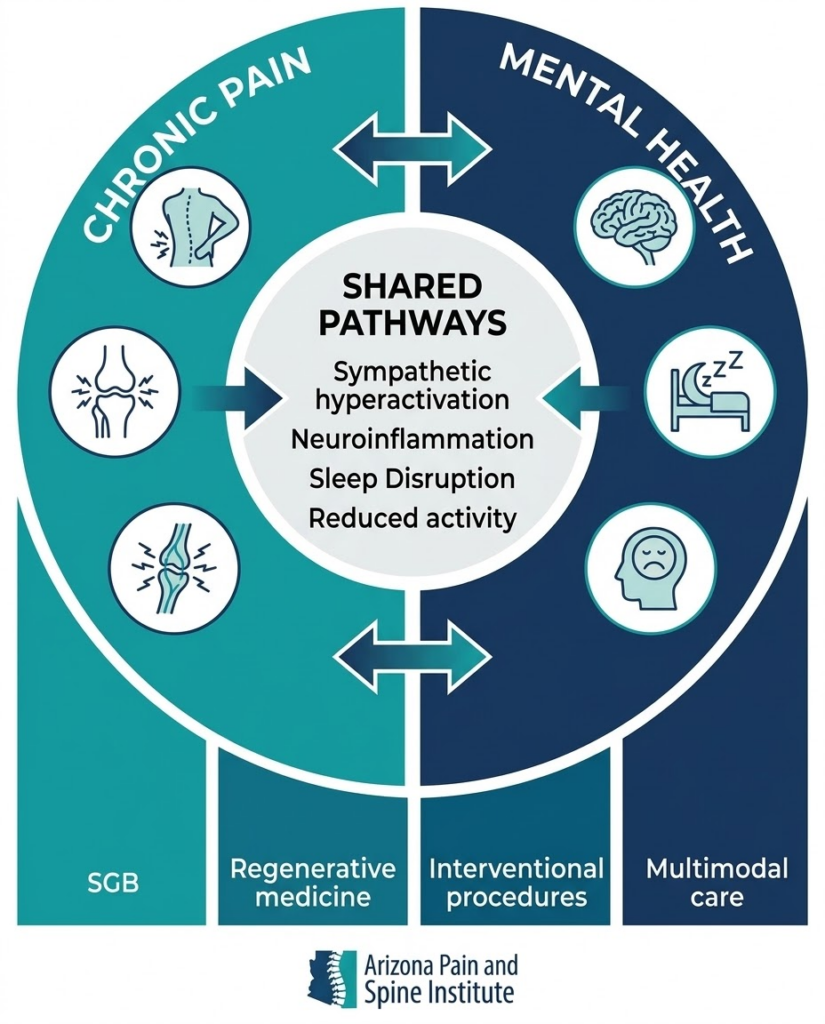
Shared Brain Pathways
Chronic pain and depression/anxiety share overlapping neural circuits. Brain regions involved in pain processing — including the anterior cingulate cortex, prefrontal cortex, and insula — are the same regions implicated in mood regulation and anxiety. When chronic pain persistently activates these circuits, it can dysregulate emotional processing. Conversely, when depression or anxiety is present, these circuits amplify pain signals, lowering the threshold at which stimuli are perceived as painful.
Sympathetic Nervous System Hyperactivation
The body’s fight-or-flight system — the sympathetic nervous system — plays a central role in both chronic pain and anxiety/PTSD. When this system remains chronically activated, it produces widespread effects: elevated heart rate, muscle tension, sleep disruption, difficulty concentrating, and heightened pain sensitivity. This is precisely the mechanism targeted by the stellate ganglion block, which Arizona Pain and Spine Institute uses to treat both PTSD/anxiety and pain-related sympathetic dysfunction.
Neuroinflammation
Emerging research identifies neuroinflammation — inflammation within the central nervous system — as a shared driver of both chronic pain and depression. Pro-inflammatory cytokines that are elevated in chronic pain conditions are the same molecules implicated in treatment-resistant depression. This creates a self-reinforcing cycle: pain drives inflammation, inflammation worsens mood, and worsened mood amplifies pain perception.
Sleep Disruption
Chronic pain disrupts sleep. Poor sleep worsens both pain sensitivity and mental health symptoms. The JAMA Network Open meta-analysis noted that sleep disruption is one of the most common bridges between physical and psychological symptoms in chronic pain populations.
How Treating Only Pain — Or Only Mental Health — Falls Short
The traditional healthcare model separates pain management from mental health treatment. A patient with chronic back pain sees a pain specialist. If they also have depression or anxiety, they’re referred to a separate psychiatrist or therapist — often with a waitlist of weeks or months, a different medical record system, and no coordination between providers.
This fragmented approach fails for several well-documented reasons. The JAMA Network Open meta-analysis authors explicitly recommended “routine screening for mental health symptoms in clinical settings where people with chronic pain are treated,” noting that this is essential to address the problem’s scale. The University of Arizona PAIN study found that people with co-occurring chronic pain and anxiety/depression accessed mental health care at lower rates than people with mental health conditions alone — suggesting that pain management settings may be the primary (and sometimes only) opportunity to identify and address these patients’ mental health needs.
For patients, this fragmentation means months of bouncing between providers, repeating their medical history, and receiving treatments that address only half the problem. A patient receiving excellent epidural injections for back pain may continue to suffer if their anxiety is amplifying their pain signals. A patient taking antidepressants for depression may find their mood improving but their pain unchanged — because the structural source of their pain hasn’t been addressed.
How Arizona Pain and Spine Institute Approaches Both Sides
Arizona Pain and Spine Institute’s model is fundamentally different from the fragmented approach. The practice treats both chronic pain conditions (lower back pain, neck pain, sciatica, neuropathy, knee pain, shoulder pain, hip pain) and mental health conditions (PTSD, anxiety) within the same clinical framework, with the same physicians, in the same locations.
Comprehensive Evaluation — 60+ Minutes for a Reason
The practice’s comprehensive initial evaluations are designed to assess the whole patient — not just the physical pain. As Dr. Ryklin has described, these evaluations focus on understanding “not just where you hurt, but how your pain affects your life.” This means evaluating sleep quality, mood changes, anxiety symptoms, activity limitations, and how long the patient has been living with pain — all factors that research shows significantly affect treatment outcomes.
Treatments That Address Both Dimensions
Arizona Pain and Spine Institute offers a range of treatments that span the physical-mental health spectrum:
Stellate ganglion block directly targets the sympathetic nervous system — the shared biological pathway between chronic pain and anxiety/PTSD. The practice’s SGB work for PTSD is backed by a Level 1B randomized controlled trial published in JAMA Psychiatry (113 service members), and the same mechanism addresses the sympathetic hyperactivation that amplifies chronic pain. The 285-patient anxiety study by Lynch et al. (2023) demonstrated a 50% reduction in GAD-7 anxiety scores following SGB — directly relevant for chronic pain patients whose anxiety is worsening their pain experience.
Interventional pain procedures — including epidural steroid injections, nerve pain injections, and radiofrequency ablation — address the structural and inflammatory sources of pain. When pain is reduced, the neurobiological cascade that drives anxiety and depression often begins to reverse. The 2024 Frontiers in Neurology meta-analysis of epidural steroid injections documented reduced opioid usage — relevant because opioid use itself is associated with worsening depression.
Regenerative medicine targets tissue-level healing rather than symptom suppression. The practice’s amniotic tissue biotechnology aims to address the root cause of pain — particularly relevant for patients with chronic conditions like knee osteoarthritis or degenerative disc disease where ongoing tissue damage perpetuates both pain and the psychological burden.
The Multimodal Philosophy
Dr. Khan has stated on the practice’s website that “a doctor who only offers one type of treatment is like a carpenter with just one tool.” For the 40% of chronic pain patients who also have depression or anxiety, this philosophy is especially critical. An effective treatment plan might combine SGB (addressing sympathetic hyperactivation and anxiety), epidural injections (reducing acute pain and inflammation), physical therapy coordination (improving function and reducing catastrophizing), and regenerative medicine (supporting long-term tissue healing) — all managed by the same clinical team.
Signs That Your Pain May Be Affecting Your Mental Health
Based on the validated screening criteria used in the JAMA Network Open meta-analysis and the University of Arizona study, chronic pain patients should pay attention to the following patterns:
- Persistent feelings of sadness, hopelessness, or loss of interest in activities you previously enjoyed — especially if these feelings developed or worsened after your pain began
- Increased anxiety, worry, or a sense of dread that feels disproportionate to your current situation
- Sleep disruption — difficulty falling asleep, staying asleep, or waking unrefreshed — that doesn’t improve even when pain is temporarily managed
- Social withdrawal or avoiding activities because of pain or because of how pain makes you feel emotionally
- Difficulty concentrating or making decisions — sometimes called “pain brain” — which overlaps significantly with anxiety-related cognitive symptoms
- Feeling that your pain treatments aren’t working as well as they should, despite addressing the physical source — which may indicate that psychological amplification is contributing to the pain experience
If you recognize several of these patterns, it doesn’t mean you’re “making up” your pain or that your pain is “all in your head.” It means your nervous system is doing exactly what the research predicts: linking physical and emotional experience through shared biological pathways.
How to Take the Next Step
For chronic pain patients in Mesa, Gilbert, Queen Creek, Chandler, Scottsdale, and Tempe who suspect their mental health may be affecting their pain — or vice versa:
- Schedule a Comprehensive Evaluation: Contact Arizona Pain and Spine Institute at (480) 986-7246 or visit gotpainarizona.com. The 60+ minute evaluation is designed to assess both physical and psychological dimensions of your pain.
- Be Honest About the Full Picture: When you meet with Dr. Khan or Dr. Ryklin, share not just your pain symptoms but how you’re sleeping, how your mood has changed, and what activities you’ve stopped doing. This information directly shapes the treatment plan.
- Ask About Integrated Options: Specifically ask about treatments that address both pain and anxiety/mood — such as stellate ganglion block, which targets the sympathetic nervous system pathway shared by chronic pain and anxiety.
- Use the FastTrack Program if Needed: For patients who cannot wait for standard scheduling — especially those experiencing significant emotional distress alongside their pain — the FastTrack cash-pay program provides expedited access.
Conclusion
The JAMA Network Open meta-analysis of 376 studies and 347,468 patients made it clear: approximately 40% of adults with chronic pain live with clinically significant depression or anxiety, and these conditions amplify each other through shared neurobiological pathways. The University of Arizona study confirmed that this co-occurrence is five times more common among people with chronic pain than without — and that it significantly worsens functional outcomes.
Arizona Pain and Spine Institute’s ability to treat both chronic pain conditions and mental health conditions like PTSD and anxiety within the same practice — using an integrated approach that includes stellate ganglion block, interventional pain procedures, and regenerative medicine — directly addresses what the research identifies as the most critical gap in chronic pain care. The next step is a conversation that addresses the whole picture. Call (480) 986-7246 or schedule through gotpainarizona.com.
Frequently Asked Questions
1. How common is depression in chronic pain patients?
A 2025 JAMA Network Open meta-analysis of 376 studies and 347,468 patients found that 39.3% of adults with chronic pain have clinically significant depression. A University of Arizona PAIN study found co-occurring symptoms are five times more common in people with chronic pain.
2. Can treating pain improve anxiety and depression?
Yes. When the structural or inflammatory source of pain is effectively addressed, the neurobiological cascade that drives anxiety and depression often begins to reverse. The 2024 Frontiers in Neurology ESI meta-analysis also documented reduced opioid usage, which is independently associated with improved mood.
3. Does Arizona Pain and Spine Institute treat anxiety and PTSD?
Yes. The practice lists both PTSD and anxiety as dedicated conditions treated and offers stellate ganglion block — backed by a Level 1B RCT published in JAMA Psychiatry — as a direct treatment. SGB targets the sympathetic nervous system, the shared pathway between chronic pain and anxiety.
4. Do I need a mental health diagnosis to be seen for pain?
No. Arizona Pain and Spine Institute is a pain management practice that evaluates the whole patient. The 60+ minute comprehensive evaluation assesses both physical and emotional aspects of your condition. If mental health symptoms are affecting your pain experience, the treatment plan will address both dimensions.
5. What should I tell my doctor about my mental health during a pain appointment?
Share everything: how your mood has changed since your pain began, sleep quality, anxiety levels, activities you’ve stopped doing, and whether you feel your current treatments address the full picture. This information directly informs treatment decisions and helps the physicians develop the most effective plan.
Disclaimer: This article references publicly available information from Arizona Pain and Spine Institute (gotpainarizona.com), JAMA Network Open (Aaron et al., 2025), CDC National Center for Health Statistics NCHS Data Brief No. 518 (November 2024, based on NHIS 2023), MMWR (Rikard et al., 2023), PAIN journal (De La Rosa et al., University of Arizona, 2024), JAMA Psychiatry (Rae Olmsted et al., 2020), ScienceDaily, and published practice information, including peer-reviewed systematic reviews, meta-analyses, government surveillance data, and clinical studies dated 2020–2025.
All metrics and study findings are from documented, peer-reviewed sources. The JAMA Network Open meta-analysis also noted that most people with chronic pain do not have depression or anxiety, and the findings “challenge the narrative that chronic pain is inherently depressing.” Results described are specific to the study populations mentioned and may vary based on individual circumstances. This article is not a substitute for professional mental health evaluation. If you are experiencing a mental health crisis, contact the 988 Suicide and Crisis Lifeline by calling or texting 988. For current information about treatments offered at Arizona Pain and Spine Institute, consult gotpainarizona.com or call (480) 986-7246.