
The largest cohort study of radiofrequency ablation for chronic low back pain ever published — 1,236 procedures analyzed in Pain and Therapy (March 2025) by Abd-Elsayed et al. at the University of Wisconsin — found a 60.6% average reduction in pain scores among successfully treated patients, with 14% of patients achieving complete pain remission. For the 23% of adults worldwide who suffer from chronic lower back pain, and for the millions of Americans for whom medications, physical therapy, and standard injections have provided only temporary relief, RFA represents a treatment that can extend pain relief from weeks to months — and in many cases, over a year. At Arizona Pain and Spine Institute in Mesa, Dr. Asim Khan and Dr. Daniel Ryklin perform radiofrequency ablation as part of their comprehensive approach to chronic back and neck pain, offering patients a proven step between short-acting injections and surgical intervention.
What Radiofrequency Ablation Is — And How It Differs From Injections
Radiofrequency ablation is a minimally invasive procedure that uses thermal energy (heat) to create a targeted lesion on specific nerves that transmit pain signals from the spine. Unlike steroid injections — which reduce inflammation temporarily — RFA disrupts the nerve’s ability to send pain signals altogether, providing substantially longer-lasting relief.
The most common application is for facet joint pain, which arises from the small joints that connect each vertebra in the spine. The nerves that supply these joints are called medial branch nerves, and they are the target of lumbar and cervical RFA. When these nerves are ablated, the brain no longer receives the pain signals from the inflamed or degenerative facet joint — even though the joint itself hasn’t changed. The nerves eventually regenerate (typically over 6–18 months), at which point the procedure can be repeated if needed.
A 2025 prospective real-world study published in Interventional Pain Medicine (the RAPID study by Provenzano et al.) enrolled 193 patients with chronic lumbar facetogenic pain and found that over 80% had been living with chronic low back pain for at least two years. Over 85% had moderate-to-crippling disability at baseline as measured by the Oswestry Disability Index. These are patients for whom conservative treatments had already failed — exactly the population that RFA is designed to serve.
The Evidence: What Large Studies Show About RFA Outcomes
The Largest-Ever RFA Cohort: 1,236 Procedures (Pain and Therapy, 2025)
The most comprehensive RFA outcomes data published to date comes from Abd-Elsayed et al. at the University of Wisconsin, published in Pain and Therapy in March 2025. This retrospective analysis reviewed 1,236 cooled radiofrequency ablation (CRFA) procedures performed between 2015 and 2024 for chronic lumbar facet pain. Among the key findings:
Get Back Your Normal Life Again
As pain specialists, we can guarantee that we are more than qualified in alleviating your pain and treating your condition.
- 60.6% average reduction in pain scores among successfully treated patients
- 14.1% of patients achieved complete remission of their pain
- Results were consistent with the therapeutic range established by prior systematic reviews
- Adverse effects were reported in only 42 of 1,450 procedures (2.9%), with the most common complaint being temporary pain during or immediately after the procedure
The RAPID Study: Real-World Prospective Data (Interventional Pain Medicine, 2025)
The RAPID (Real-world Assessment of Prospective outcomes In patients treated with lumbar radiofrequency ablation for chronic pain) study by Provenzano et al. enrolled 193 patients across multiple sites from December 2020 to January 2024. Critically, 97.9% of enrolled patients had undergone diagnostic medial branch blocks prior to RFA, with 99.5% reporting at least 50% relief and 95.8% reporting at least 80% relief — confirming the diagnostic precision that predicts RFA success. The study tracked outcomes through 18 months, providing some of the longest prospective follow-up data available.
Meta-Analysis: Placebo-Controlled Evidence (Radiology and Medicine, 2024)
A 2024 systematic review and meta-analysis published in Radiology and Medicine by Láinez Ramos-Bossini et al. specifically examined placebo-controlled randomized controlled trials of RFA for lumbar facet joint pain. The meta-analysis confirmed the efficacy of radiofrequency ablation over sham procedures, providing Level I evidence that the treatment effect is not simply due to placebo response.
24-Month Comparative Study (Journal of Clinical Medicine, 2025)
A 2025 single-center retrospective cohort study published in the Journal of Clinical Medicine compared radiofrequency ablation (97 patients) to cryoablation (83 patients) over 24 months. RF ablation yielded earlier and more significant improvements in function and pain relief lasting up to 18 months, with overall benefits maintained through the 24-month follow-up period.
The Three-Step Process: How RFA Works at Arizona Pain and Spine Institute
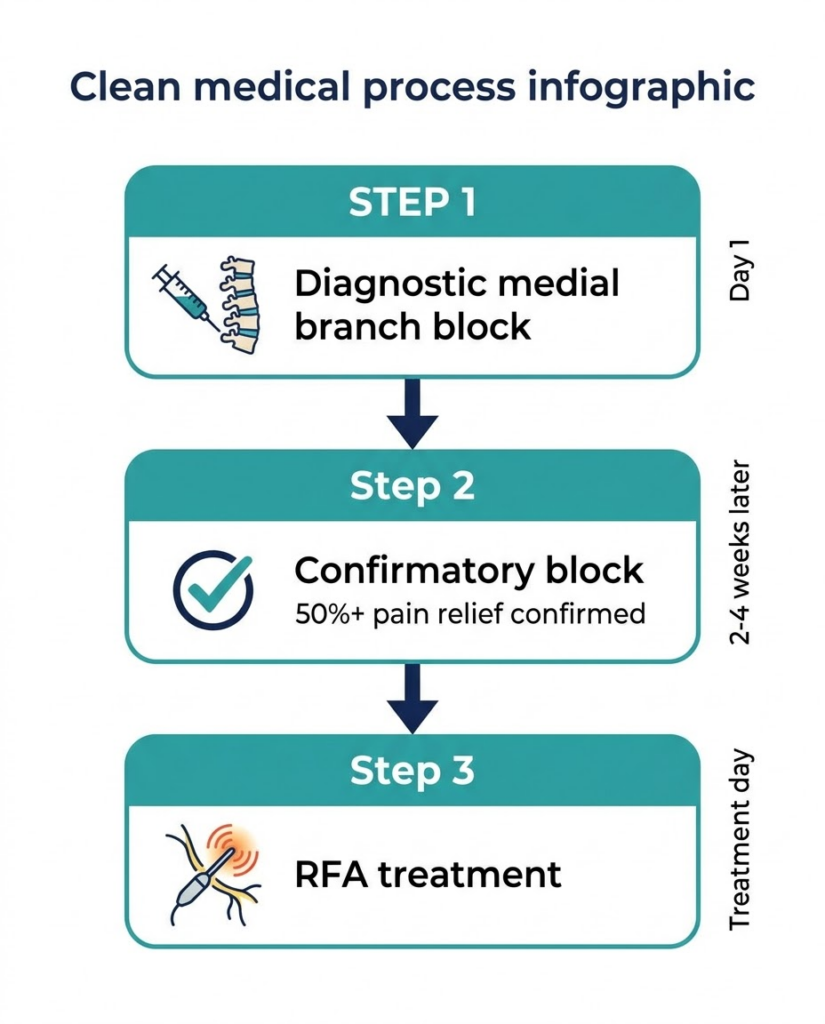
One of the most important things patients should understand about radiofrequency ablation is that it follows a rigorous multi-step diagnostic process. This isn’t a treatment that’s performed on the first visit — and practices that skip the diagnostic steps typically see lower success rates.
Step 1: Diagnostic Medial Branch Block
Before RFA is ever performed, the physician must first confirm that the facet joints are actually the source of the patient’s pain. This is done through a diagnostic medial branch block — a small injection of local anesthetic near the medial branch nerves under fluoroscopic guidance. If the patient experiences significant pain relief (typically defined as 50% or greater improvement) during the hours after the block, this confirms that the targeted nerves are transmitting the pain signals.
The RAPID study documented that 99.5% of patients who underwent diagnostic blocks prior to RFA reported at least 50% relief — demonstrating why this diagnostic step is critical for predicting treatment success.
Step 2: Confirmatory Block
Many insurance protocols and best-practice guidelines require a second confirmatory medial branch block before proceeding to RFA. This ensures that the first block’s results were not a false positive. Dr. Khan and Dr. Ryklin follow evidence-based protocols that prioritize diagnostic accuracy — because performing RFA on the wrong nerve level wastes time and resources while delaying effective treatment.
Step 3: Radiofrequency Ablation
Once the pain-generating nerves are confirmed through the diagnostic process, the RFA procedure itself is performed. At Arizona Pain and Spine Institute, this involves:
Positioning: The patient lies face-down on a procedure table. The treatment area is cleaned and locally anesthetized.
Needle Placement: Using fluoroscopic (live X-ray) guidance, the physician positions a specialized radiofrequency needle adjacent to the targeted medial branch nerve. The most commonly treated levels are L3/4, L4/5, and L5/S1 in the lumbar spine, as documented in the RAPID study.
Testing: Before ablation, the physician performs sensory and motor testing through the needle to confirm proper placement — ensuring the needle is near the correct sensory nerve and safely away from motor nerves.
Ablation: Thermal energy is delivered through the needle, creating a controlled lesion at a temperature of approximately 80°C for 60–90 seconds (the RAPID study found that 84% of patients were treated with a 90-second lesion time at 80°C). This disrupts the nerve’s ability to transmit pain signals.
Recovery: The procedure is performed on an outpatient basis. Patients may experience some local soreness at the treatment sites for several days to two weeks. Most patients notice meaningful pain reduction within 2–4 weeks as the ablated nerve tissue fully heals.
How Long Does Radiofrequency Ablation Last?
This is the question patients ask most frequently, and the answer is supported by substantial data. The nerves targeted by RFA eventually regenerate — but this process takes months.
Based on the published evidence, patients can expect pain relief lasting 6 to 18 months following a successful RFA procedure. The 2025 Journal of Clinical Medicine 24-month comparative study found that RF ablation provided significant functional improvements maintained through 18 months, with both study groups showing the need for retreatment strategies beyond that point. The largest-ever CRFA cohort study documented a mean relief duration consistent with this range, though 14.1% of patients achieved complete remission.
When pain returns — indicating nerve regeneration — the procedure can be repeated. Many patients undergo RFA on an annual or semi-annual basis as part of an ongoing pain management strategy. The practice’s comprehensive evaluation process helps determine the optimal retreatment timeline for each patient.
Where RFA Fits in the Treatment Ladder
Dr. Khan has emphasized that effective pain management requires a multimodal toolbox. Radiofrequency ablation occupies a specific and important position in the treatment hierarchy at Arizona Pain and Spine Institute:
Before RFA — shorter-acting options: Epidural steroid injections and nerve pain injections provide weeks to months of relief and are often the first interventional step. If a patient responds well to medial branch blocks but finds the relief too short-lived (wearing off in days to weeks), RFA is the logical next step to extend that relief to months.
Alongside RFA — complementary treatments: Physical therapy, activity modification, and the practice’s regenerative medicine options can be combined with RFA for a comprehensive approach. Dr. Ryklin’s background in Physical Medicine and Rehabilitation makes him particularly skilled at integrating RFA with rehabilitation strategies.
After RFA — if more is needed: For patients whose pain is refractory to RFA or who have pain generators beyond the facet joints, advanced options like spinal cord stimulation may be considered. The practice’s published content on SCS provides continuity for these patients.
What Patients Should Realistically Expect
Success rates: The 1,236-procedure CRFA study found a 60.6% average pain reduction among successfully treated patients. The RAPID study’s rigorous diagnostic protocol (99.5% diagnostic block responders) suggests that proper patient selection is the key predictor of success.
Timeline: Most patients notice meaningful improvement within 2–4 weeks. Maximum benefit typically develops by 6–8 weeks post-procedure.
Duration: 6–18 months is the typical range, with retreatment available when pain returns.
Safety: The largest CRFA cohort reported adverse effects in only 2.9% of procedures. Common post-procedure experiences include localized soreness and muscle spasm at the treatment site, which typically resolve within one to two weeks.
What RFA does not do: RFA does not repair the underlying degenerative joint disease. It provides sustained pain relief by interrupting the nerve signals — giving patients months of improved function, reduced medication use, and better quality of life while the underlying condition is managed through complementary approaches.
How to Get Started
For chronic back or neck pain patients in Mesa, Gilbert, Queen Creek, Chandler, Scottsdale, and Tempe:
- Schedule a Consultation: Contact Arizona Pain and Spine Institute at (480) 986-7246 or visit gotpainarizona.com. The FastTrack cash-pay program is available for expedited access.
- Comprehensive Evaluation: During the 60+ minute initial evaluation, Dr. Khan or Dr. Ryklin will assess whether your pain pattern is consistent with facet joint origin — the primary indication for RFA.
- Diagnostic Block: If facet joint pain is suspected, a diagnostic medial branch block will be performed under fluoroscopic guidance to confirm the pain source.
- Treatment: Following successful diagnostic blocks, RFA is scheduled as an outpatient procedure — typically taking 30–60 minutes depending on the number of levels treated.
Conclusion
The 1,236-procedure CRFA cohort study, the 193-patient RAPID prospective study, the 2024 placebo-controlled meta-analysis, and the 24-month comparative data collectively demonstrate that radiofrequency ablation is an evidence-based, effective treatment for chronic facet-mediated back and neck pain — delivering 60%+ pain reduction that lasts 6–18 months with a strong safety profile. For chronic pain patients who have found temporary relief from injections but need longer-lasting results without surgery, RFA fills a critical gap.
Arizona Pain and Spine Institute’s fluoroscopy-guided approach, rigorous diagnostic protocol, and multimodal treatment philosophy ensure that RFA is delivered within the evidence-based framework that produces the best outcomes. Call (480) 986-7246 or schedule through gotpainarizona.com.
Frequently Asked Questions
1. How long does the radiofrequency ablation procedure take?
The RFA procedure itself typically takes 30–60 minutes depending on the number of spinal levels treated. It is performed on an outpatient basis at Arizona Pain and Spine Institute, and patients go home the same day.
2. Is radiofrequency ablation painful?
Local anesthesia is used to numb the treatment area before the procedure. Patients may feel pressure or mild discomfort during ablation. Post-procedure soreness at the treatment sites is common and typically resolves within one to two weeks.
3. How many levels can be treated with RFA at once?
The RAPID study found that most patients underwent RFA at two facet joint levels, most commonly L3/4, L4/5, and L5/S1. Dr. Khan and Dr. Ryklin determine the number of levels based on diagnostic block results and each patient’s individual anatomy.
4. Can radiofrequency ablation be repeated?
Yes. Because the targeted nerves regenerate over 6–18 months, RFA can be repeated when pain returns. Many patients undergo the procedure annually as part of an ongoing pain management strategy.
5. Does insurance cover radiofrequency ablation?
Most insurance plans cover RFA for facet joint pain when the diagnostic medial branch block protocol has been completed. Arizona Pain and Spine Institute also offers the FastTrack cash-pay program. Contact (480) 986-7246 for coverage details.
Disclaimer: This article references publicly available information from Arizona Pain and Spine Institute (gotpainarizona.com), Pain and Therapy (Abd-Elsayed et al., March 2025), Interventional Pain Medicine/RAPID study (Provenzano et al., 2025), Radiology and Medicine (Láinez Ramos-Bossini et al., 2024), Journal of Clinical Medicine (2025), and StatPearls/National Library of Medicine, including peer-reviewed studies, prospective and retrospective analyses, systematic reviews, and published practice information dated 2020–2025. All metrics and study findings are from documented, peer-reviewed sources. RFA outcomes depend on accurate diagnosis through the medial branch block protocol; patients who do not respond to diagnostic blocks are not candidates for RFA. The 2025 CRFA study reported a 60.6% average pain reduction among successfully treated patients; individual results may vary. Results described are specific to the study populations mentioned and may vary based on individual circumstances, diagnosis, pain severity, and treatment adherence. For current information about treatments offered at Arizona Pain and Spine Institute, consult gotpainarizona.com or call (480) 986-7246.